





Опыт лечения переломов надколенника с применением артроскопии у детей
- Авторы: Тимофеев И.В.1, Дьяконова Е.Ю.1, Гусев А.А.1, Романова Е.А.1, Хроленко П.В.1
-
Учреждения:
- ФГАУ «Научный центр здоровья детей» Минздрава России
- Выпуск: Том 5, № 1 (2017)
- Страницы: 53-57
- Раздел: Статьи
- Статья получена: 01.04.2017
- Статья одобрена: 01.04.2017
- Статья опубликована: 31.03.2017
- URL: https://journals.eco-vector.com/turner/article/view/6158
- DOI: https://doi.org/10.17816/PTORS5153-57
- ID: 6158

Цитировать

Аннотация
Введение. По литературным данным, частота переломов надколенника составляет примерно от 0,5 до 1,5 % от всех повреждений скелета. По характеру перелома можно выделить авульзивные, поперечные, оскольчатые и продольные. При смещении фрагментов более 2–3 мм и повреждении сухожильного растяжения четырехглавой мышцы предпочтительна открытая репозиция с восстановлением конгруэнтности суставной поверхности и стабильным остеосинтезом. В случаях продольных переломов артроскопия может рассматриваться как высокоэффективный метод хирургического лечения.
Материалы и методы. С применением артроскопии нами были прооперированы 4 пациента с продольным переломом надколенника. Возрастной диапазон пострадавших варьировал от 14 до 17 лет. Из них 3 мальчика и 1 девочка. Все больные получили травму во время занятий спортом.
Поскольку при продольных переломах надколенника боковой разгибательный аппарат четырехглавой мышцы бедра оставался неповрежденным, объем оперативного вмешательства в этих случаях заключался в артроскопически ассистированной закрытой репозиции фрагментов и чрескожной диафиксации спицами без наложения проволочного шва.
Результаты и обсуждение. Малоинвазивность, возможность визуального контроля за качеством восстановления геометрии суставной поверхности надколенника и надежностью фиксации фрагментов, существенное сокращение сроков последующей реабилитации делают артроскопию высокоэффективным методом хирургического лечения переломов надколенника.
Ключевые слова
Полный текст
Введение
Переломы надколенника относительно редки у детей [1]. По литературным данным, частота переломов надколенника составляет примерно от 0,5 до 1,5 % от всех повреждений скелета. Надколенник в какой-то мере защищает коленный сустав спереди. Но в то же время его передняя подкожная локализация делает его уязвимым для прямой травмы, такой, как удар колена о приборную панель автомобиля или падение на переднюю часть колена [2]. Непрямой механизм перелома наступает при резком и внезапном, насильственном сокращении четырехглавой мышцы бедра [2, 3], поэтому обстоятельства травмы — это, как правило, занятия спортом и дорожно-транспортные происшествия [3].
По характеру можно выделить авульзивные, поперечные, продольные и оскольчатые переломы [4].
Для детей характерны авульзивные переломы нижнего или верхнего полюса. Они встречаются более чем в половине случаев переломов надколенника. Затем следуют поперечные переломы, реже всего встречаются оскольчатые [4–6]. Отличительной особенностью таких переломов является частое сочетание перелома с разрывом медиального и латерального сухожильных растяжений четырехглавой мышцы бедра. Продольные переломы встречаются реже всего. При этих переломах редко бывает нарушение бокового разгибательного аппарата [2].
Поскольку надколенник играет решающую роль в механизме разгибания в коленном суставе, целью любого лечения являются восстановление геометрии суставной поверхности надколенника и стабильная фиксация фрагментов [5]. В противном случае вероятность развития пателло-феморального артроза и, как следствие, нарушения функции коленного сустава существенно возрастает [1, 3].
Характер перелома, наличие и степень смещения фрагментов определяются после рентгенологического обследования.
Переломы надколенника со смещением отломков, не превышающим 2–3 мм, и минимальной инконгруэнтностью свидетельствуют о целостности разгибательного аппарата. В этих случаях консервативное лечение позволяет добиться положительных результатов. Чаще всего такой подход применим при авульзивных переломах, когда степень смещения фрагментов невелика [1, 5–7].
Переломы со смещением более 2–3 мм, как правило, сопровождаются повреждением сухожильного растяжения четырехглавой мышцы и несостоятельностью разгибательного аппарата. Их лечение заключается в открытой репозиции, восстановлении конгруэнтности и стабильном остеосинтезе, дополненном швом сухожильного растяжения (бокового разгибательного аппарата квадрицепса). Необходимость в оперативном лечении возникает в случаях поперечных, оскольчатых и продольных переломов [2, 5, 7].
Мнения относительно оптимальных методов оперативного лечения переломов надколенника расходятся. Принятые методики включают большое количество стягивающих проволочных швов, использование винтов, в том числе канюлированных, частичной или тотальной пателлэктомии с выполнением при этом шва либо пластики разгибательного аппарата. Характер и объем вмешательства определяются исходя из конкретной ситуации [7, 8].
Недостатком открытых репозиций являются травматичность и сложность контроля за восстановлением конгруэнтности суставной поверхности, что является одной из ключевых позиций, влияющих на восстановление функции сустава. Для достижения наиболее точного сопоставления фрагментов требуется рентгенологический контроль. При этом состояние хрящевого покрова оценить сложно [2, 7, 9, 10].
Артроскопия в сочетании с чрескожным остеосинтезом лишена этих недостатков. Малоинвазивность и визуальный контроль на этапах закрытой репозиции и фиксации фрагментов вызывают несомненный интерес, а в случае интактности медиального и латерального сухожильных растяжений четырехглавой мышцы позволяют рассматривать артроскопию как метод выбора хирургической коррекции [8, 10].
Важным этапом лечебного процесса у пациентов с переломами надколенника представляется послеоперационный период с последующей реабилитацией и восстановлением функции сустава. Согласно публикациям, посвященным как открытым, так и артроскопическим методам хирургического лечения, консолидация перелома наступала через 6–7 недель независимо от метода лечения [11–13]. Что касается восстановления функции сустава, в публикациях, посвященных открытым методикам, авторы отмечают сохраняющиеся функциональные нарушения на протяжении 8–12 недель [13], а в ряде случаев — до 12 месяцев [12]. В то же время другие авторы отмечают, что применение артроскопии позволяет сократить сроки реабилитационного периода до 6 недель, признавая артроскопическую внутреннюю фиксацию допустимой альтернативой для лечения при переломах надколенника со смещением [8, 11].
Материалы и методы
В течение 3 лет (2013–2015) с применением артроскопии были прооперированы 4 пациента с продольным переломом надколенника. Все пациенты добровольно подписали информированное согласие на участие в исследовании и выполнение хирургического вмешательства.
Возрастной диапазон пострадавших варьировал от 14 до 17 лет. Из них 3 мальчика и 1 девочка. Все больные получили травму во время занятий спортом.
При первичном осмотре у всех пациентов на первый план выступала клиника гемартроза коленного сустава. Поскольку данные клинического осмотра, результатов лучевой диагностики, интраоперационные артроскопические находки у всех пациентов носили идентичный характер, мы решили проиллюстрировать свои наблюдения на примере одного пациента.
Больной М., 16 лет, госпитализирован с клиникой гемартроза левого коленного сустава.
Рентгенография коленного сустава в прямой и боковой проекциях оказалась неинформативной. Костно-травматических изменений на рентгенограммах выявлено не было (рис. 1, а, б).
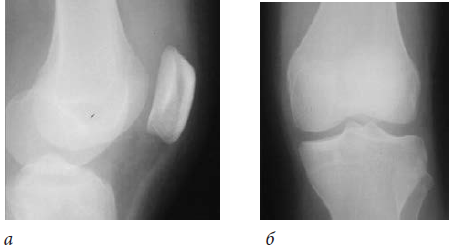
Рис. 1. Больной М., 16 лет. Рентгенография левого коленного сустава: а — боковая проекция; б — прямая проекция
После выполнения пункции коленного сустава и иммобилизации осуществлен повторный клинический осмотр. В ходе осмотра обращала на себя внимание сохраняющаяся выраженная локальная болезненность в проекции надколенника.
В связи с этим спектр диагностических мероприятий был расширен и выполнены ультразвуковое исследование и компьютерная томография коленных суставов (рис. 2, 3).

Рис. 2. Больной М., 16 лет. УЗ-исследование коленных суставов. Выявлен перелом левого надколенника
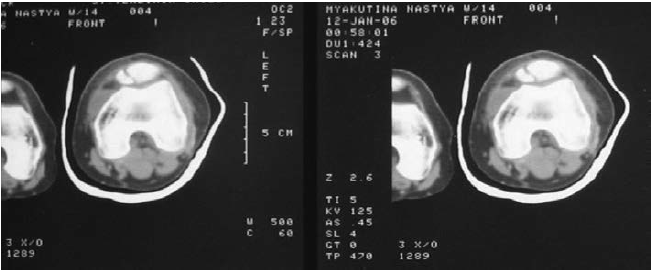
Рис. 3. Больной М., 16 лет. Компьютерная томография коленных суставов. Определяется продольный перелом левого надколенника
Результаты расширенного обследования позволили выявить продольный перелом надколенника.
Для оценки состояния хрящевого покрова надколенника первым этапом хирургического лечения была выполнена диагностическая артроскопия. Исследование проводили из стандартного антеро-латерального доступа в жидкостной среде. Артроскопическая картина у всех пациентов была идентичной. В случаях продольного перелома надколенника фрагменты подвижны и нестабильны, суставная поверхность инконгруэнтна (рис. 4).

Рис. 4. Больной М., 16 лет. Артроскопия левого коленного сустава. Продольный перелом надколенника со смещением
При этом медиальное и латеральное сухожильные растяжения четырехглавой мышцы не пострадали. Интраоперационные находки позволили выполнить одномоментно под видеоконтролем репозицию фрагментов. Репозиция внутрисуставно осуществлялась с помощью артроскопического крючка, проведенного через антеро-медиальный доступ с одновременным ручным пособием снаружи (рис. 5).
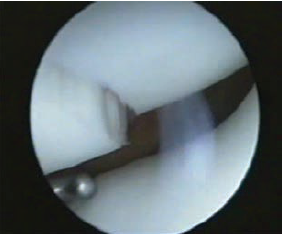
Рис. 5. Больной М., 16 лет. Этап репозиции фрагментов надколенника под артроскопическим контролем
После сопоставления фрагментов последние удерживались в репонированном состоянии и одновременно выполнялся чрескожный остеосинтез двумя спицами. Спицы проводились в горизонтальной плоскости под углом около 45 градусов друг к другу. Проволочный шов не накладывался. Видеоконтроль позволил убедиться в стабильности остеосинтеза (рис. 6).

Рис. 6. Больной М., 16 лет. После устранения деформации суставной поверхности надколенника выполнена чрескожная фиксация фрагментов
В послеоперационном периоде выполнялась иммобилизация в гипсовом туторе сроком на 6 недель. Реабилитацию начинали с четвертой недели после операции. Это первый период реабилитации, который длился 2 недели. В это время пострадавший еще носит гипсовую лонгету, поэтому все упражнения выполняются стоя на костылях или лежа. После консолидации перелома, прекращения иммобилизации и удаления металлофиксаторов начинали второй курс реабилитации сроком 2 недели с целью ликвидации постиммобилизационной тугоподвижности коленного сустава. Завершением реабилитационного периода был возврат к прежнему уровню физических нагрузок. В общей сложности длительность реабилитации составляла 6 недель.
Результаты и обсуждение
Анализ клинических данных, результатов лучевой диагностики и лечебно-диагностической артроскопии показал, что при продольных переломах надколенника лечебно-диагностический алгоритм имеет некоторые особенности. Может оказаться недостаточной информативность традиционной рентгенографии. Наложение рентгенологической тени надколенника на тень мыщелкового комплекса бедренной кости в прямой проекции и наслоение теней фрагментов надколенника в боковой проекции увеличивают вероятность диагностической ошибки. Поэтому в спектр диагностических мероприятий целесообразно включить УЗ-исследование и компьютерную томографию коленных суставов. После постановки диагноза хирургическое вмешательство целесообразно начинать с лечебно-диагностической артроскопии. Это дает возможность визуально оценить состояние хрящевого покрова как надколенника, так и бедренной кости, убедиться в интактности разгибательного аппарата квадрицепса и под видеоконтролем выполнить репозицию фрагментов в сочетании с чрескожным металлоостеосинтезом. В случае сохранности связок, удерживающих надколенник, чрескожный остеосинтез в достаточной степени стабилен и позволяет избежать наложения дополнительных проволочных швов. Малотравматичность артроскопии дает возможность раннего начала реабилитации, еще до прекращения иммобилизации, что сокращает период восстановления функции сустава.
Длительность катамнестического наблюдения составила от 1,5 до 4 лет. Оценка результатов лечения производилась с применением шкалы субъективной оценки коленного сустава IKDC. Среднее значение было 92,3 (от 87,3 до 96,5). Во всех случаях удалось добиться восстановления функции сустава и возвращения к прежнему уровню физических нагрузок. Это позволяет рассматривать артроскопию в сочетании с чрескожным остеосинтезом как высокоэффективный метод хирургического лечения.
Таким образом, малоинвазивность, возможность полного визуального контроля за качеством восстановления геометрии суставной поверхности надколенника и надежности фиксации фрагментов, сокращение сроков последующей реабилитации и выгодный косметический результат делают применение артроскопии при лечении больных с переломами надколенника оправданным и целесообразным.
Информация о финансировании и конфликте интересов
Работа произведена на базе и при поддержке ФГАУ «НЦЗД» МЗ РФ. Авторы декларируют отсутствие явных и потенциальных конфликтов интересов, связанных с публикацией настоящей статьи.
Об авторах
Игорь Викторович Тимофеев
ФГАУ «Научный центр здоровья детей» Минздрава России
Автор, ответственный за переписку.
Email: doctor_timofeev@mail.ru
канд. мед. наук, врач травматолог-ортопед отделения хирургии
РоссияЕлена Юрьевна Дьяконова
ФГАУ «Научный центр здоровья детей» Минздрава России
Email: doctor_timofeev@mail.ru
канд. мед. наук, заместитель главного врача по хирургии
РоссияАлексей Андреевич Гусев
ФГАУ «Научный центр здоровья детей» Минздрава России
Email: doctor_timofeev@mail.ru
канд. мед. наук, заместитель начальника отдела хирургии
РоссияЕкатерина Алексеевна Романова
ФГАУ «Научный центр здоровья детей» Минздрава России
Email: doctor_timofeev@mail.ru
врач-хирург отделения хирургии
РоссияПолина Владимировна Хроленко
ФГАУ «Научный центр здоровья детей» Минздрава России
Email: doctor_timofeev@mail.ru
врач-ординатор отделения хирургии
РоссияСписок литературы
- Schmal H, Strohm PC, Niemeyer P, et al. Fractures of the patella in children and adolescents. Acta Orthop Belg. 2010;76(5):644-50. doi: 10.1007/s00167-012-2036-0.
- Galla M, Lobenhoffer P. Patella fractures. Chirurg. 2005;76(10):987-97. doi: 10.1007/s00104-005-1081-3.
- Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg. 2011;19(4):198-207. doi: 10.5435/00124635-201104000-00004.
- Dai LY, Zhang WM. Fractures of the patella in children. Knee Surg Sports Traumatol Arthrosc. 1999;7(4):243-5. doi: 10.1007/s001670050156.
- Springorum HP, Siewe J, Dargel J, et al. Classification and treatment of patella fractures. Orthopade. 2011;40(10):877-80. doi: 10.1007/s00132-011-1780-z.
- Gao GX, Mahadev A, Lee EH. Sleeve fracture of the patella in children. J Orthop Surg (Hong Kong). 2008;16(1):43-6. doi: 10.1177/230949900801600111.
- Kakazu R, Archdeacon MT. Surgical management of patellar fractures. Orthop Clin North Am. 2016;47(1):77-83. doi: 10.1016/j.ocl.2015.08.010.
- El-Sayed AM, Ragab RK. Arthroscopic-assisted reduction and stabilization of transverse fractures of the patella. Knee. 2009;16(1):54-7. doi: 10.1016/j.knee.2008.07.010.
- Harty J, Byrne S, Kenny P, et al. Single screw fixation of a patellar sleeve rupture: a case report. Eur J Orthop Surg Traumatol. 2002;12:48. doi: 10.1007/s00590-002-0010-0.
- Maeno S, Hashimoto D, Otani T, et al. A novel surgical technique for patellar fracture: application of extra-articular arthroscopy with hanger-lifting procedure. Arthrosc Tech. 2013;2(3):e275-e279. doi: 10.1016/j.eats.2013.03.002.
- Makino A, Aponte-Tinao L, et al. Arthroscopic-assisted surgical technique for treating patella fractures. Arthroscopy. 2002;18(6):671-5. doi: 10.1053/jars.2002.30745.
- Lazaro LE, Wellman DS, Sauro G, et al. Outcomes after operative fixation of complete articular patellar fractures: assessment of functional impairment. J Bone Joint Surg Am. 2013;95(14):e961-8. doi: 10.2106/JBJS.L.00012.
- Malik M, Halwai MA. Open reduction and internal fixation of patellar fractures with tension band wiring through cannulated screws. J Knee Surg. 2014;27(5):377-82. doi: 10.1055/s-0033-1364100.
Дополнительные файлы

